At the American Society of Cataract and Refractive Surgery meeting in May, I reported on the results of four prospective, multicenter clinical investigations of Abbott Medical Optics’ Tecnis Symfony IOL, a new presbyopia-correcting IOL that merges two complementary technologies — an echelette design and achromatic technology — to provide an extended range of continuous vision.
The studies were conducted at 69 sites in the United States, New Zealand and Europe, with 3- to 6-month follow-up of 1,464 eyes of 735 subjects. In each of the studies, patients were randomized to bilateral implantation of either the Symfony lens (ZXR00) or a monofocal control lens (ZCB00). Subjects and evaluators were masked to the IOL implanted.
Study results
Distance visual acuity was comparable in the monofocal and Symfony groups. The Symfony groups had significantly better near and intermediate acuity. There were consistently low reports of visual symptoms: About 90% of subjects across both IOL groups reported no or only mild halos (Figure 1), more than 93% of subjects reported no or only mild glare, and more than 95% reported no or only mild starbursts.
The symptom questionnaires were non-directed — that is, at most sites, subjects were asked if they had experienced any difficulties or problems with their eyes or vision since their last visit. If they had symptoms, they were then asked to specify which symptoms (glare, halo, starbursts) and to rate each symptom as mild, moderate or severe. Twelve European sites asked a more directed question: “Do you experience any glare or halo at any time during the day or night?” Directed questionnaires usually result in higher reports of symptoms, but we found little difference in glare and halo reports between the European study with some directed questionnaires and the other studies.
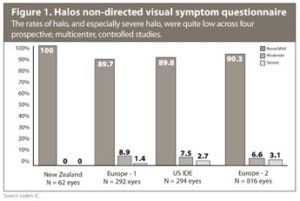
Most subjects who reported symptoms rated them as mild or moderate. In the U.S. study, for example, reports of severe visual symptoms were less than 2.8% for halos, none for glare and less than 1.5% for starbursts.
Historically, we have seen that 3% to 5% of patients implanted with monofocal aspheric lenses report glare and halo, so there is only a small increase in these studies. It is important to note that the use of femtosecond laser, manual limbal relaxing incisions, and LASIK or PRK enhancement were all disallowed during the study, so residual sphere or cylinder error may also have contributed to the incidence of visual symptoms.
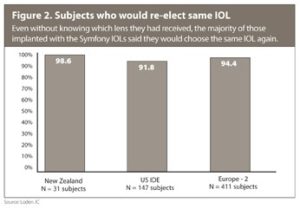
In the European studies, subjects were asked if they would recommend the lens to a friend. Nearly all (97.9% in the Europe-1 study and 93.7% in the Europe-2 study) said yes. A high percentage of patients across studies said they would choose to have the same IOL implanted again (Figure 2). This level of satisfaction is particularly noteworthy given the design of the study. Because patients did not know whether they were getting the monofocal lens or the extended range of vision IOL, they were not counseled about neuroadaptation to the lens or the need to use good light. Surgeons did not attempt to set expectations as we typically would when implanting a presbyopia-correcting IOL.
Personal experience
I personally treated 24 patients in the study, including 11 who received the Symfony lens.
I was pleasantly surprised by how good their near vision was. The mean near acuity was approximately 20/30 in the U.S. trial, and my patients found that they rarely needed reading glasses for normal-sized print in room lighting.
I have not seen the visual symptom data analyzed by refractive error, but my guess is that those with moderate to severe halo or glare are more likely to have been those who needed an enhancement. Certainly that was the case in my practice. Two of my patients who were not fully satisfied initially needed an enhancement after the study was completed.
