“I was told that I have astigmatism.”
This is a common phrase that eye doctors hear from their patients, especially when they present for LASIK or cataract surgery. Sometimes it’s even phrased “an astigmatism” like an object of some kind. Although most of these patients are familiar with the term and are aware that it affects their vision and glasses prescription in some way, many are still not exactly sure what it is and how it will affect their future treatment options. So what exactly is it? Will it be there forever? And if affects vision, how can it be treated?
Astigmatism… Sounds like some sort of affliction or disease to some people, but this is, of course, not the case. Rest assured, astigmatism is not a disease or a major abnormality. In fact, almost everyone has at least some amount of measurable astigmatism. In the simplest terms, astigmatism can be thought of as a way of describing the shape and the focusing characteristics of the eye, in particular, the very front part of the eye called the cornea. The best way to fully understand it is to start with the eye’s anatomy.
The Cornea
The human eye actually shares many characteristics of a camera. The front part of the eye focuses the incoming light while the neurological film in the back of the eye, called the retina, captures the image. The cornea actually does most of the eye’s focusing. When the shape of the cornea is not perfectly symmetrical, it is described as having astigmatism. And that means that it will not focus light symmetrically in all directions. Let’s examine a few basic lessons about the eye’s optics.
The cornea is remarkable because it is the only transparent tissue in the entire body. Although it may seem to be merely a clear window for the eye, it actually serves several very important functions. One of those functions is to bend or refract incoming light just like the lens of a camera so that a sharp image can be focused on the retina. This process is called refraction. The natural lens inside the eye also serves in this function, and together, these two structures help us see clearly.
In the ideal situation, the focusing power of the cornea and natural lens will coincide with the size or axial length of the eye. This would mean that the eye would be in perfect focus all the time without the need for refractive aides like glasses or contacts. But as we all know, this is not always the case. In fact, it is estimated that about 75% of American adults use some form of vision correction.
The curvature and shape of the cornea is what determines its focusing power. This curvature is measured in diopters (D), similar to the measurement in eyeglasses. A steeper or more curved cornea will have a higher diopter power, while a flatter cornea will have a lower diopter power. The average cornea curvature measures around 44-45 D, but can range anywhere between 40 and 50D typically. The higher the diopter power, the stronger the focus. That means that light refracted by a 44D cornea will come into focus at a closer range compared to that of a 42D cornea.
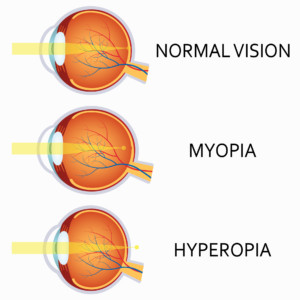 When a person has a corneal focusing power that is too strong for the length of the eye, the light will come into focus before it reaches the retina. This causes nearsightedness or myopia, the most common form of blurred vision requiring glasses. The opposite is true for people with farsightedness or hyperopia. Their focusing power is not strong enough and the focal point falls somewhere past the retina. A nearsighted person will need eyeglasses with a minus (-) or negative prescription to help decrease the focusing power of the eye while a farsighted person will need a plus (+) or positive prescription to add power.
When a person has a corneal focusing power that is too strong for the length of the eye, the light will come into focus before it reaches the retina. This causes nearsightedness or myopia, the most common form of blurred vision requiring glasses. The opposite is true for people with farsightedness or hyperopia. Their focusing power is not strong enough and the focal point falls somewhere past the retina. A nearsighted person will need eyeglasses with a minus (-) or negative prescription to help decrease the focusing power of the eye while a farsighted person will need a plus (+) or positive prescription to add power.
The axial length of the eye also plays a key role. This is the distance from the anterior tip of the cornea to the center of the retina in the back of the eye. All of us have different axial lengths as well as different cornea powers. The shorter the axial length of an eye, the more corneal power it needs to be in focus. The opposite is true for a longer eye, which would need less corneal power. Two separate individuals could have the same exact cornea curvature and yet have completely different glasses prescriptions because one has an eye that is much longer or shorter than the other.
Where does astigmatism come into play?
As mentioned above, astigmatism can be thought of as a form of asymmetry. Both the cornea and the natural lens can have astigmatism, but the amount that is measured in the cornea is usually far more significant. In terms of corneal shape, astigmatism means that the diopter curvature of the cornea is steeper in one direction compared to another. The easiest way to visualize this concept is to think of the surface of a football. The long axis of the football has a flatter curve than the shorter axis and these two curvatures are 90 degrees apart. In a much less dramatic sense, this is how the surface of a cornea with astigmatism is shaped.
Here’s a quick example: In ophthalmology, as a person looks straight ahead, the imaginary horizontal line that would bisect the cornea into two equal halves is said to be at the 180° axis or meridian. The imaginary vertical line is the 90° axis. Let’s say that when a person has their cornea curvature measured in the horizontal meridian it measures 42D. However, in the vertical meridian, it measures 45D. That would mean that this person has 3D of corneal astigmatism. From a focusing standpoint, this means that the cornea will focus light more strongly in the vertical meridian than it does in the horizontal. So in a sense, the cornea has two separate focusing powers that are 90° apart based on its shape  and curvature. This example demonstrates a fairly significant amount of astigmatism. However, the magnitude of astigmatism can range to very small amounts, such as 0.5D, to very large amounts that are 5D or more. As mentioned above, most corneas will have at least some measurable astigmatism and it is rare to come across a cornea that is perfectly symmetrical in all meridians. Visually, even small amounts astigmatism can be significant.
and curvature. This example demonstrates a fairly significant amount of astigmatism. However, the magnitude of astigmatism can range to very small amounts, such as 0.5D, to very large amounts that are 5D or more. As mentioned above, most corneas will have at least some measurable astigmatism and it is rare to come across a cornea that is perfectly symmetrical in all meridians. Visually, even small amounts astigmatism can be significant.
 In most instances of astigmatism, called with-the-rule astigmatism, the vertical meridian is steeper than the horizontal, but this is certainly not always the case. When the horizontal meridian is steeper, that is termed against-the-rule astigmatism. The steep meridian can actually be at any angle between 0 and 180°. The corresponding flat meridian is typically 90° away unless the cornea has some sort of pathological irregularity. So if a person’s steep axis is measured to be at the 60° axis, the flattest curvature will be at the 150° axis. This person would be said to have an oblique astigmatism.
In most instances of astigmatism, called with-the-rule astigmatism, the vertical meridian is steeper than the horizontal, but this is certainly not always the case. When the horizontal meridian is steeper, that is termed against-the-rule astigmatism. The steep meridian can actually be at any angle between 0 and 180°. The corresponding flat meridian is typically 90° away unless the cornea has some sort of pathological irregularity. So if a person’s steep axis is measured to be at the 60° axis, the flattest curvature will be at the 150° axis. This person would be said to have an oblique astigmatism.
So how does an eye with astigmatism get into focus?
There are several ways, but all of them involve balancing out or neutralizing astigmatism. One way is with the use of astigmatism correcting lenses. The most common form of this is the typical pair of eyeglasses. These lenses can be shaped and manufactured to counterbalance the eye’s astigmatism simply by having an astigmatic shape that is equal in magnitude to the eye’s astigmatism, but in the opposite direction. Think of the cornea as being a football that is standing upright and the glasses as being an identical football lying on its side in front of the first one.
If you look at a typical glasses prescription, you will see three separate numbers for each eye. One simple example would be -2.00 -1.50 x 180, let’s say for a left eye. The second number (in this case the -1.50 ) represents that amount or magnitude of the eye’s astigmatism and the third number (180) represents the axis of that astigmatism. So in this example, the person’s left eye is nearsighted (-2.00) and needs 1.5D of astigmatism correction.
Now does this mean that this person has exactly 1.5D of astigmatism or curvature difference in the cornea? Not necessarily, and this is where it can get a little tricky. We have been talking mostly about corneal astigmatism, but it is important to again mention the fact that the natural lens inside the eye can also have asymmetry or astigmatism. This is called lenticular astigmatism. However, as God’s great design would have it, in most cases astigmatism that is present in the natural lens actually counterbalances the cornea astigmatism, at least to some degree. That means that if the cornea is steeper in the vertical meridian, the lens will often be steeper in the horizontal meridian, reducing the actual focusing difference between the two meridians. Therefore it is possible for a person to have, let’s say, 2D of corneal astigmatism, but only need 0.75D of astigmatism correction in their glasses because the eye’s natural lens has balanced out 1.25D. This 0.75D of astigmatism correction in the glasses prescription represents what we call refractive astigmatism. This concept becomes particularly important in the setting of cataract surgery, which we discuss in detail below.
Correcting Astigmatism
LASIK Surgery
These days, there are certainly many choices when it comes to correcting astigmatism. For many, glasses or contacts work very well and provide a convenient and comfortable option for clear vision. However, for some, these options may not work as well. With glasses, the astigmatism correction can create some visual distortion and loss of depth perception. This is especially true when patients are looking down or off to the side through the periphery of the lens. These symptoms are often exacerbated when bifocals are added to the prescription.
Contacts that correct astigmatism are called toric contact lenses and are quite popular, especially for those that have at least 1.0 D of astigmatism correction. Unlike regular contact lenses, toric contacts have to oriented in a precise way so that the astigmatism can be corrected properly. To do this, these lenses are weighted to be slightly heavier on the bottom to minimize rotation. Despite their tremendous success, these lenses can be quite challenging to fit and can occasionally rotate, leading to intermittent blurred vision. These symptoms can be quite frustrating.
It is for reasons like these, among others, that patients with astigmatism will often explore other options to correct their vision, namely LASIK surgery. LASIK has become more popular than ever and has proven its safety and efficacy for almost 3 decades now! The Patient Reported Outcome studies (PROWL 1 & 2) that were published in 2014 by the FDA show overwhelmingly positive results, with over 96% reporting satisfaction with their vision at 3 months following LASIK. 1 And more recently, a very unique and thorough study published in the journal of Ophthalmology in October of 2016 compared symptoms and visual satisfaction between patients who had LASIK and patients that continued to wear glasses and contacts. It concluded that “Compared with contact lens wear, current LASIK technology improved ease of night driving, did not significantly increase dry eye symptoms, and resulted in higher levels of satisfaction at 1, 2, and 3 years follow-up.” 2
However, it is still quite surprising to see how many people still put off being evaluated for LASIK because they are under the impression that LASIK cannot correct astigmatism. This is simply not the case. In fact the vast majority of custom LASIK procedures correct at least some degree of astigmatism. It is true that very high prescriptions of all kinds, myopic, hyperopic, and astigmatism, can fall outside of the range that can be corrected with LASIK. However, with modern LASIK platforms like the iDesign advanced wavescan system, surgeons can now treat up to 5D of astigmatism!
The precision of the preoperative iDesign mapping of over 1,200 data points, along with the precise alignment of the VISX Star 4 Laser with iris registration, allows for tremendously accurate results, with over 98% of our myopic patients, including those with astigmatism, achieving a visual result of 20/20 or better! And because there is no longer a shifting contact lens or distorted peripheral vision from glasses, the patients’ satisfaction with their vision is often higher than they had ever previously achieved in their lives.
Cataract Surgery
The same amount of satisfaction is also very commonly seen after cataract surgery. People often express concern and disbelief when their doctors tell them that they have cataracts. But did you know that a cataract is simply the natural lens inside the eye that has undergone the normal aging process? In doing so, it has become more dense and yellow, blocking light and causing reduced vision with glare. All of us will get cataracts in our lifetime if we live long enough.
Although cataract surgery used to involve less refined techniques, a stay in the hospital, higher risks, and variable results, today, it is a 10-15 minute outpatient procedure with very low risk and tremendous visual outcomes. In fact, cataract surgery can be looked upon these days as not just a medical procedure, but rather an opportunity to get out of glasses and enjoy spectacle free vision. That is an opportunity that many people have never in their lives had the chance to experience. And this is true even for people with astigmatism.
How is this possible? As mentioned above, the natural lens is a major focusing component of the eye along with the cornea. When cataract surgery is performed, what is essentially taking place is that the eye’s natural lens is being removed and replaced with an Intraocular Lens Implant or IOL. Therefore, the optics, or the focusing power of the eye is being adjusted or changed. Calculations are made before the surgery to choose the IOL power that will put the eye in the sharpest focus. With modern techniques and formulas, the visual results fall with in 0.5D of intended outcome 75% of the time.
But what if you have astigmatism? When the natural lens is removed and the IOL is inserted inside the eye, the optics of the cornea, including its existing astigmatism, are relatively left unchanged. That means, if left uncorrected, this astigmatism will cause a significant amount of blurriness for both distance and near objects. In most cases, a pair of bifocal spectacles will correct this.
But what if you don’t want to wear spectacles?
Fortunately, there are options which will allow the surgeon to correct astigmatism at the time of the cataract surgery, significantly decreasing, and in some cases, eliminating the need for spectacle correction.
The first way that this is done is by utilizing what are called arcuate incisions or limbal relaxing incisions (LRIs). This technique is used to correct smaller amounts of astigmatism that are typically less than 1 D. During the surgery, small curved partial thickness incisions are made near the outer border of the cornea, centered on the steep axis. These incisions cause a flattening affect that reduces that asymmetry of the corneal shape and allows for better focus. Today, surgeons can utilize specialized cataract lasers like the Lensar to make these incisions as accurate and symmetrical as possible, increasing the chances of success.
For larger degrees of astigmatism, special lens implants called Toric lens implants (similar to the toric contacts) are a much better option. Most lens implants have a single or spherical power only, with no astigmatism correction. This means that the best they can do for a person with astigmatism is to average out the two powers of the cornea and simply split the difference.
Let’s look at an oversimplified example: Say that in a given eye with a symmetrical cornea of 43D, the perfect IOL to achieve the best focus would be 20D. Or if the cornea measured 41D instead, the perfect IOL would be 22D. If that same eye were to not have a symmetrical cornea, but rather astigmatism with the steep curvature of 43D and a flat curvature of 41D, then neither one of these implants would work well. Only one axis would be in focus at a time while the other would be quite blurry. The best choice for a spherical lens, in this case, would be one that averages the two powers. Theoretically, in this example, that would be a 21D lens. This would be better, but still, neither axis would be in perfect focus and glasses would definitely be necessary to sharpen the vision. Again this example is a bit oversimplified but certainly illustrates the basic concepts.
 Toric lens implants, on the other hand, do have the astigmatism correction built into them. When they are used at the time of cataract surgery, they are aligned along the steep axis of the astigmatism to neutralize the asymmetrical focus.
Toric lens implants, on the other hand, do have the astigmatism correction built into them. When they are used at the time of cataract surgery, they are aligned along the steep axis of the astigmatism to neutralize the asymmetrical focus.
This results in a much higher visual quality after surgery due to the fact the astigmatism is corrected inside the eye.
This means there is no longer the visual distortion associated with astigmatism eyeglasses or fluctuations due to rotating contact lenses. In addition, most patients with these lenses no longer need glasses for any of their distance related activities like driving, watching TV, or playing sports! Some of our happiest patients are those that have opted for toric lenses implants.
What’s even more exciting is that there are now toric lens implants like the Symfony Toric, from Abbott Medical Optics that also have multifocal optics. When used for the right patients, these lenses provide spectacle freedom for not only distance activities, but also for most intermediate and near tasks!
In some cases, toric lens implants may even be the right choice for people who have never had significant astigmatism. How can this be? The answer is the lenticular astigmatism that was discussed earlier. That is the astigmatism that is present in the natural lens of the eye that often offsets the corneal astigmatism. When a cataract patient shows a lot of corneal astigmatism on their preoperative measurements, but very little refractive astigmatism in their glasses, that means that their natural lens is neutralizing or balancing out the corneal astigmatism. Now, when this person has cataract surgery and the natural lens is removed, the corneal astigmatism will manifest itself and will cause a significant amount of blurriness if a spherical IOL is used instead of a toric. As you can imagine, this can lead to some pretty dissatisfied patients who now have to get used to a pair of astigmatism correcting spectacles that they never needed in the past.
So, hopefully, this discussion has illustrated just how important (and sometimes confusing) astigmatism and its management can be.
Fortunately, with the technology and the expertise that is now available, we no longer have to let astigmatism limit our vision or our options when it comes to seeing our world clearly.
References:
- Eydelma MB et al. Listening to the Patients—The Laser-Assisted In Situ Keratomileusis Quality of Life Collaboration Project. JAMA Ophthalmol. 2017;135(2):83-84.
- Price MO et al. Three-Year Longitudinal Survey Comparing Visual Satisfaction with LASIK and Contact Lenses. Ophthalmology. 2016 Aug;123(8):1659-66.
